

Very Good Overview of COVID-19
 04-21-2020, 09:14 PM
04-21-2020, 09:14 PM
#1
Gets Weekends Off
Thread Starter
Joined APC: Dec 2017
Position: Retired NJA & AA
Posts: 1,916
A very balanced and rational look the COVID-19 virus. If you want to see the charts go to the website:
https://erinbromage.wixsite.com/covi...8cIzZ5pQklb_O4
A long but very interesting read. The author has a Ph.D. in Biology and his research includes:
*The role of long-lived plasma cells in immunological memory
* Antibody secreting cell diversity following vaccination and infection
* Modeling the adaptation of the B-cell response following immunization
The Virus: SARS-CoV2. Severe Acute Respiratory Syndrome Coronavirus 2
The Disease SARS-CoV2 can cause: COVID-19. Coronavirus Disease of 2019
Genetically Engineered Virus: NO. This virus was not manufactured in a lab with bits and pieces from other viruses put into its backbone. People based this on a poorly written paper, that found 15 nucleotides in a similar order to a sequence found in HIV. This is 15 nucleotides out of 30,000 in the viral genome. Further analysis, by qualified scientists, showed that this 'finding' was an artifact of the alignment method used by the authors (i.e the authors screwed up and the paper was withdrawn).
A wild-type virus being studied in a lab that escaped: Impossible to rule this out right now, but it‘s not the most likely origin. In full disclosure, there was a virology lab in Wuhan that was working on bat coronaviruses. They collected bats to study from an area roughly 40 miles outside of Wuhan. The (single) Chinese scientists was working in collaboration with scientists from North Carolina on a NIH R01 grant for $3.7 million that ran from 2014-2019. There are many bat coronaviruses and from their published work, this SARS-CoV2 was not genetically similar to isolates they were studying.
A wild-virus that spilled-over into humans: Given that CoV has jumped from animal hosts to human at least 2 times previously (SARS 2003 and MERS 2006 - ongoing), and that the genome of this virus is similar to BatRaTG13 coronavirus, and even closer in similarity to a virus isolated from pangolins. The most logical outcome is that this was a natural spillover event. When and where it happened, we don't know.
https://www.nature.com/articles/s41591-020-0820-9
Over the next 2 weeks, scientist from the Wuhan Institute of Virology (and others) reported people with a severe pneumonia being admitted to ICU.
Doctors started sampling bronchoalveolar fluid on December 24th to try and isolate the infectious agent. By December 30th, the first partial genome sequence of the virus was released internally to the Chinese CDC, it wrongly classifying the virus as SARS (the 2003 version). Worried doctors started sharing this information privately.
By January 1st 2020, only 250 or so people had the infection. On the same day, the WHO and US CDC Director were briefed by the Chinese CDC director about a severe but unknown viral outbreak.
On January 3rd, China formally notified the USA of the outbreak.
On January 5th, the Chinese CDC submitted the complete genome of the virus isolated from sick patients.
From isolation of an unknown virus to a complete genomic sequence was less than 2 weeks.
In the period, January 1st through the 15th. There were a lot of mixed messages and unknowns about the virus and how it was transmitted. At this stage only 2 people had died, and they were not certain of human-to-human transmission yet.
On January 16th a molecular diagnostic test was developed by German Scientists and adopted worldwide, including by WHO.
It appears the first case of this new virus entered the USA on or around January 15th. It is estimated that ~45 people brought the virus into the USA between Jan 15th-30th, most were dead end infections (they fizzled out), and only a few of those infected people (~9) started outbreaks in the USA (Washington, California, and New York). This information is based off the genetic sequencing and analysis being run on Nextstrain.org.
Countries around the world, started confirming cases in late January (Australia, Malaysia, Japan, Hong Kong, UK, Russia, basically, everywhere that looked).
First cases in the USA were diagnosed in the last week of January.
By January 30th, the 10th update from WHO was given, declaring the outbreak an PHEIC (Public Health Emergency of International Concern). This new virus joined other active PHEIC's; Ebola and Polio. The WHO designated that COVID-19 risk to the world was high.
January 31st: US closed its borders to people who had visited China in the past 14 days. This definitely helped stop more seeding events from Mainland China.
Late January into February, the outbreak in China escalated, taking until mid-March to control.
Basically, we know with a high degree of certainty that the outbreak originated from a single spillover event in China, in November, it spread at low levels until early December, and then hit a sentinel population mid December resulting in hospitalizations. The virus, through movement of people, moved from Wuhan to the rest of the world over the next 30 days. The initial seeding event in the USA was around January 15th. With many more seeding events occurring in February from infected people coming from Europe.
Bottom line, nope, your sickness last year was something else.
RT-rPCR: this was the molecular test designed by the German Scientist in January. Basically, you collect a sample, using a swab, from the very very back of your nose (nasopharangeal). In that sample, you have your own cells, and if you are infected, the virus as well. The virus is then extracted from the sample (Bust cells, wash away crud, capture nucleic acids, and then collect pure nucleic acids fro analysis. We then have to convert the viral RNA to DNA. Following this step a pair of primers and a probe are used to amplify any detect any viral genetic material. These primers/probe are VERY specific and will only amplify a specific part of the genome of this virus. For a more detailed description see here https://virologydownunder.com/kits-r...s-and-viruses/
Basically, if this test comes back positive, it means you are currently infected with SARS-CoV2. It does not mean you have COVID-19, which is the disease the virus CAN cause.
We have currently done about 3 million of these tests in the USA. The test can be done in 15 minutes (Roche POC test), but typically takes 24-48 hours when you are having to process 100-1000's of samples at a time.
Antigen Test: This is the new test coming to market soon. It basically uses antibodies, which have been made in the lab, to detect viral proteins in your mucus and spit. It works just like a pregnancy test, but with spit rather than pee. There is the potential that millions of these tests can be made available per week. They can be done at home, or if done in a hospital or doctors surgery, they are much safer for the staff.
If this test comes back positive, it means you are currently infected with SARS-CoV2. It does not mean you have COVID-19, which is the disease the virus CAN cause
Serological test (Antibody test): These tests are available now. Serological tests determine if you have been PREVIOUSLY infected. They test your blood to see if you have antibodies that recognize proteins found on the surface of the virus. At the moment, these tests are highly problematic. Too many unverified tests coming in from overseas. If the manufacturer has designed it wrong, it will give you a false positive reading. It will signal that you were infected, but in reality you are still susceptible.
If this test comes back positive, and it works properly, it means you were previously infected SARS-CoV2. PLEASE NOTE: That more than 50% of all diagnosis coming from these serological test, even the best designed ones, will give you a false positive reading.Tread very carefully with making life decisions based on outcomes of this test (For now).
When you are infected with one of the 4 standard human coronaviruses (ones that cause the common cold), you develop immunity for a few months but then immunity wanes. That is why you can get another cold the next year.
However, if you were infected and then recovered from either MERS or SARS infections, you developed a protective immunity that lasts for at least 2-3 years.
Initial data with SARS-CoV2 suggests you have immunity for at least a few months. Data with primates suggests that you can't be reinfected in the first few months after recovery. But we do not know how long it last.
We need to keep watching this space: there are reports of people in South Korea, 163 people to be exact, testing positive to SARS-CoV2 months after recovering.
By the USA numbers, 5.3% of those people diagnosed by the molecular test with SARS-CoV2, die. That is a terrifying number. But that number is clearly wrong. It's too high.
There are many people who are mildly sick, who can't get a test. And we know, that there are many people who get infected but never show symptoms (asymptomatic). So while the number of deaths is a fairly robust measurement, the number of people infected is not.
As of the time of writing this, we have 755,162 people diagnosed with SARS-CoV2 infections in the USA. It is more likely that 5-25 million people have already been infected. At the outside maybe 1% of the population of the USA. At that level, the mortality rate is approaching what is seen during a bad flu season.
But there are some huge caveats that go with this assessment of disease severity
https://erinbromage.wixsite.com/covi...8cIzZ5pQklb_O4
A long but very interesting read. The author has a Ph.D. in Biology and his research includes:
*The role of long-lived plasma cells in immunological memory
* Antibody secreting cell diversity following vaccination and infection
* Modeling the adaptation of the B-cell response following immunization
Where we are now?
This is a longer post than usual. Sort of where we came from and where we are. I try to address a few conspiracies, rumors etc. I cover the origins of the virus, some testing, if i'm infected am I immune, and is it as deadly as they say.The Virus: SARS-CoV2. Severe Acute Respiratory Syndrome Coronavirus 2
The Disease SARS-CoV2 can cause: COVID-19. Coronavirus Disease of 2019
Origins of the Virus:
No one knows for certain, but there is strong evidence that this was a natural spillover event (animals to humans).Genetically Engineered Virus: NO. This virus was not manufactured in a lab with bits and pieces from other viruses put into its backbone. People based this on a poorly written paper, that found 15 nucleotides in a similar order to a sequence found in HIV. This is 15 nucleotides out of 30,000 in the viral genome. Further analysis, by qualified scientists, showed that this 'finding' was an artifact of the alignment method used by the authors (i.e the authors screwed up and the paper was withdrawn).
A wild-type virus being studied in a lab that escaped: Impossible to rule this out right now, but it‘s not the most likely origin. In full disclosure, there was a virology lab in Wuhan that was working on bat coronaviruses. They collected bats to study from an area roughly 40 miles outside of Wuhan. The (single) Chinese scientists was working in collaboration with scientists from North Carolina on a NIH R01 grant for $3.7 million that ran from 2014-2019. There are many bat coronaviruses and from their published work, this SARS-CoV2 was not genetically similar to isolates they were studying.
A wild-virus that spilled-over into humans: Given that CoV has jumped from animal hosts to human at least 2 times previously (SARS 2003 and MERS 2006 - ongoing), and that the genome of this virus is similar to BatRaTG13 coronavirus, and even closer in similarity to a virus isolated from pangolins. The most logical outcome is that this was a natural spillover event. When and where it happened, we don't know.
https://www.nature.com/articles/s41591-020-0820-9
Was my Sickness in November/December/January CoVID-19
The data would say no. It appears the virus first jumped into humans in ~November of 2019. The first person that we know was infected with this virus was an 81 year old Chinese man with no links to the now famous Wuhan wet-market. 10 days later, a seafood merchant became sick. By December 16th there were 41 cases of a disease with unknown etiology (cause), more than half of those people sick had a link to the market. Thus, the wet market was NOT the origins of the outbreak, possibly just a site of a super-spreading event.Over the next 2 weeks, scientist from the Wuhan Institute of Virology (and others) reported people with a severe pneumonia being admitted to ICU.
Doctors started sampling bronchoalveolar fluid on December 24th to try and isolate the infectious agent. By December 30th, the first partial genome sequence of the virus was released internally to the Chinese CDC, it wrongly classifying the virus as SARS (the 2003 version). Worried doctors started sharing this information privately.
By January 1st 2020, only 250 or so people had the infection. On the same day, the WHO and US CDC Director were briefed by the Chinese CDC director about a severe but unknown viral outbreak.
On January 3rd, China formally notified the USA of the outbreak.
On January 5th, the Chinese CDC submitted the complete genome of the virus isolated from sick patients.
From isolation of an unknown virus to a complete genomic sequence was less than 2 weeks.
In the period, January 1st through the 15th. There were a lot of mixed messages and unknowns about the virus and how it was transmitted. At this stage only 2 people had died, and they were not certain of human-to-human transmission yet.
On January 16th a molecular diagnostic test was developed by German Scientists and adopted worldwide, including by WHO.
It appears the first case of this new virus entered the USA on or around January 15th. It is estimated that ~45 people brought the virus into the USA between Jan 15th-30th, most were dead end infections (they fizzled out), and only a few of those infected people (~9) started outbreaks in the USA (Washington, California, and New York). This information is based off the genetic sequencing and analysis being run on Nextstrain.org.
Countries around the world, started confirming cases in late January (Australia, Malaysia, Japan, Hong Kong, UK, Russia, basically, everywhere that looked).
First cases in the USA were diagnosed in the last week of January.
By January 30th, the 10th update from WHO was given, declaring the outbreak an PHEIC (Public Health Emergency of International Concern). This new virus joined other active PHEIC's; Ebola and Polio. The WHO designated that COVID-19 risk to the world was high.
January 31st: US closed its borders to people who had visited China in the past 14 days. This definitely helped stop more seeding events from Mainland China.
Late January into February, the outbreak in China escalated, taking until mid-March to control.
Basically, we know with a high degree of certainty that the outbreak originated from a single spillover event in China, in November, it spread at low levels until early December, and then hit a sentinel population mid December resulting in hospitalizations. The virus, through movement of people, moved from Wuhan to the rest of the world over the next 30 days. The initial seeding event in the USA was around January 15th. With many more seeding events occurring in February from infected people coming from Europe.
Bottom line, nope, your sickness last year was something else.
Testing and Diagnosis
You have heard a lot about testing and its probably getting a little confusing, Especially with the new tests coming online. So let me break them down for you.RT-rPCR: this was the molecular test designed by the German Scientist in January. Basically, you collect a sample, using a swab, from the very very back of your nose (nasopharangeal). In that sample, you have your own cells, and if you are infected, the virus as well. The virus is then extracted from the sample (Bust cells, wash away crud, capture nucleic acids, and then collect pure nucleic acids fro analysis. We then have to convert the viral RNA to DNA. Following this step a pair of primers and a probe are used to amplify any detect any viral genetic material. These primers/probe are VERY specific and will only amplify a specific part of the genome of this virus. For a more detailed description see here https://virologydownunder.com/kits-r...s-and-viruses/
Basically, if this test comes back positive, it means you are currently infected with SARS-CoV2. It does not mean you have COVID-19, which is the disease the virus CAN cause.
We have currently done about 3 million of these tests in the USA. The test can be done in 15 minutes (Roche POC test), but typically takes 24-48 hours when you are having to process 100-1000's of samples at a time.
Antigen Test: This is the new test coming to market soon. It basically uses antibodies, which have been made in the lab, to detect viral proteins in your mucus and spit. It works just like a pregnancy test, but with spit rather than pee. There is the potential that millions of these tests can be made available per week. They can be done at home, or if done in a hospital or doctors surgery, they are much safer for the staff.
If this test comes back positive, it means you are currently infected with SARS-CoV2. It does not mean you have COVID-19, which is the disease the virus CAN cause
Serological test (Antibody test): These tests are available now. Serological tests determine if you have been PREVIOUSLY infected. They test your blood to see if you have antibodies that recognize proteins found on the surface of the virus. At the moment, these tests are highly problematic. Too many unverified tests coming in from overseas. If the manufacturer has designed it wrong, it will give you a false positive reading. It will signal that you were infected, but in reality you are still susceptible.
If this test comes back positive, and it works properly, it means you were previously infected SARS-CoV2. PLEASE NOTE: That more than 50% of all diagnosis coming from these serological test, even the best designed ones, will give you a false positive reading.Tread very carefully with making life decisions based on outcomes of this test (For now).
If infected, am I Immune?
We don't know.When you are infected with one of the 4 standard human coronaviruses (ones that cause the common cold), you develop immunity for a few months but then immunity wanes. That is why you can get another cold the next year.
However, if you were infected and then recovered from either MERS or SARS infections, you developed a protective immunity that lasts for at least 2-3 years.
Initial data with SARS-CoV2 suggests you have immunity for at least a few months. Data with primates suggests that you can't be reinfected in the first few months after recovery. But we do not know how long it last.
We need to keep watching this space: there are reports of people in South Korea, 163 people to be exact, testing positive to SARS-CoV2 months after recovering.
Is it as deadly as they say?
This is tough to answer.By the USA numbers, 5.3% of those people diagnosed by the molecular test with SARS-CoV2, die. That is a terrifying number. But that number is clearly wrong. It's too high.
There are many people who are mildly sick, who can't get a test. And we know, that there are many people who get infected but never show symptoms (asymptomatic). So while the number of deaths is a fairly robust measurement, the number of people infected is not.
As of the time of writing this, we have 755,162 people diagnosed with SARS-CoV2 infections in the USA. It is more likely that 5-25 million people have already been infected. At the outside maybe 1% of the population of the USA. At that level, the mortality rate is approaching what is seen during a bad flu season.
But there are some huge caveats that go with this assessment of disease severity
- First, we don't yet know how many are infected. That needs to come from well-design and well-executed serological studies. The ones done so far are not very robust, but they do suggest that many more than the 750k people currently diagnosed have been infected.
- This virus spreads very fast. So rather than infections and deaths being spread out over a 6 month flu season, they all come in a crush. An analogy would be that a restaurant can serve 50,000 meals over a year, but the same restaurant can't fulfill 50,000 orders in a week. Most orders couldn't be fulfilled....with health care, an unfulfilled order means a death. Remember, from a flu index case, a ten-point transmission chain results in ~15 infections. While with SARS-CoV, a single index case transmission chain results in 59,000 infections.
- For the same number of infections, this virus puts 10-20x more people in hospital. Just like SARS-CoV2, influenza cases are under-counted. But of those seeking medical help, this virus requires hospital-interventions at a much higher rate.
- Dose is related to outcomes. People receiving a higher infectious dose have poorer clinical outcomes. This is why our Doctors, Nurses, and First Responders are dying. They are being exposed to the virus in their work environment in higher doses than us, and its killing them.
- There is a vaccine for influenza. If you choose to vaccinate yourself against influenza, you can either avoid or mitigate the most serious effects of an influenza infection. Even if the vaccine doesn't perfectly match the circulating strain, vaccination provides enhanced protection and better outcomes. Roughly 93% of Doctors and Nurses choose to have a seasonal flu shot to protect themself at work. They have a tool to protect themselves in the workplace against the flu. There is no such protection for them for SARS-CoV2.
- Recovery from the flu is 6-9 days. Recovery from COVID-19 is 10-30 days. Sick patients require more hospital resources for a longer period of time than an influenza case. This means more beds and more staff.
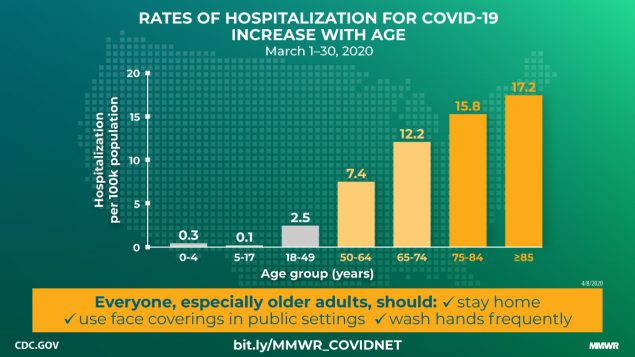
- 50% of all hospitalized patients are under the age of 50. So while most deaths currently cluster in the over 55 group, half of the hospitalizations, the ones that also need beds and Doctors and Nurses, are under the age of 50.
- Bottom line, this virus's mortality rate will be lower than the current numbers show. Blame that on the poor testing rate. But, it doesn't take away from the fact that this virus is unlike anything we have encountered in modern history. A virus that spreads fast and cryptically through our population, then due to social stratification, explodes in infections, morbidity, hospitalizations, and death. We do not have the infrastructure or the tools to handle so many people getting sick and requiring hospitalization at one time. If we just let this virus do its thing, all-cause mortality, in every age group, would be off-the-charts.
The longer this goes, the more we will know, the better prepared we will be, and the better the outcomes for the infected. We had to shut down, it was the right call. The USA has streamlined our healthcare system to the bone, we nearly have the worst citizen-to-ICU bed ratio in developed world. We just did not/do not have the capacity to deal with the hospitalizations from this virus.
And before anyone says my body, my choice to risk infection. Just like your right to throw a punch ends at my nose, your right to ignore community-wide safety precautions ends at the lungs of healthcare workers and anyone else you interact.
History will show that the shut down was the right call, it saved many lives. Did we overshoot? Probably. But we needed to overdo our response because of our lost month of testing in February. We were running blind. Lack of testing allowed the number of infected people to get so large, the peak so much higher, that descending from that peak will take much longer. That month of inaction required a disproportionately large response in March and April and will have ripple effects for the rest of the year.
But, I also believe that easing restrictions needs to happen, sooner than many other people will be comfortable. Not yet, we are not ready. Get the hospitals sorted out, get the PPE issues sorted out, get the supply-chains issue sort out, and finally get the testing we need in place. The Federal plan released last week is a good one if enacted properly. Once that is together, and our health care people are safely equipped to deal with patients, then restrictions can be gradually lifted.
Finally, even if we open the economy up tomorrow, you will have no economic recovery without customers. Restaurant patronage dropped precipitously in the month leading up to them being officially closed. Movie theaters are still open in Sweden, patronage is just 10% of normal. If your livelihood relies on customers, you are going to have to work out how to service customers who have concerns for their well-being, even if you do not have similar concerns for yourself.
 04-22-2020, 09:49 AM
04-22-2020, 09:49 AM
#2
P/T Gear Slinger
Joined APC: May 2017
Position: Airbus
Posts: 824
Originally Posted by AirBear

A very balanced and rational look the COVID-19 virus. If you want to see the charts go to the website
...
.
...
.
04-22-2020, 10:08 AM
#3
The NeverEnding Story
Joined APC: Sep 2005
Posts: 7,512
I’m not sure how on one hand the author can discuss how contagious the virus is, while on the other believing there were only 250 total worldwide cases on 1 Jan after the first case was discovered in November.
In a city as densely populated as Wuhan, within a country with as many densely populated cities as China.
Given that, I’m also not sure how the author concludes the virus first entered the US “around” 15 Jan - the first *known* case.
That said, I think its mostly even-keeled...but hey I’m just a dumb pilot, not a Ph.D in biology.
In a city as densely populated as Wuhan, within a country with as many densely populated cities as China.
Given that, I’m also not sure how the author concludes the virus first entered the US “around” 15 Jan - the first *known* case.
That said, I think its mostly even-keeled...but hey I’m just a dumb pilot, not a Ph.D in biology.
 04-22-2020, 03:56 PM
04-22-2020, 03:56 PM
#4
Gets Weekends Off
Joined APC: Jan 2018
Posts: 644
Originally Posted by BoilerUP
I’m not sure how on one hand the author can discuss how contagious the virus is, while on the other believing there were only 250 total worldwide cases on 1 Jan after the first case was discovered in November.
In a city as densely populated as Wuhan, within a country with as many densely populated cities as China.
Given that, I’m also not sure how the author concludes the virus first entered the US “around” 15 Jan - the first *known* case.
That said, I think its mostly even-keeled...but hey I’m just a dumb pilot, not a Ph.D in biology.
In a city as densely populated as Wuhan, within a country with as many densely populated cities as China.
Given that, I’m also not sure how the author concludes the virus first entered the US “around” 15 Jan - the first *known* case.
That said, I think its mostly even-keeled...but hey I’m just a dumb pilot, not a Ph.D in biology.
The other thing is that pandemics spread like a wild fire; at first they're easy to contain and often burn out on their own, but once they're going, they're really hard to stop.
04-22-2020, 04:08 PM
#5
Gets Weekends Off
Joined APC: Jun 2018
Position: Sitting
Posts: 500
Originally Posted by Duffman
My fiance is an epidemiologist and what I've learned from her is that this so incredibly complicated it's impossible to just 'common sense' through it. They do a lot of detective, boots-on-ground, knocking-on-doors type work mixed with grad level statistics and numerical methods. In other words, unless you're an epi working on this day in and day out, there's nothing we've thought of that they haven't.
The other thing is that pandemics spread like a wild fire; at first they're easy to contain and often burn out on their own, but once they're going, they're really hard to stop.
The other thing is that pandemics spread like a wild fire; at first they're easy to contain and often burn out on their own, but once they're going, they're really hard to stop.

 04-23-2020, 10:24 AM
04-23-2020, 10:24 AM
#9
Gets Weekends Off
Joined APC: Jul 2006
Posts: 194


Thread
Thread Starter
Forum
Replies
Last Post


